![]()
Pyoderma Gangrenosum
 Many of us enjoy the aspect of medicine that requires our refined detective skills to not only find clues in the haystacks of chief complaints and presentations, but also use those clues to deduce a diagnosis. It is one of the unique characteristics of emergency medicine; however, when those clues are of dermatologic origin, they can be quite tricky. We have discussed several aspects of skin lesions previously (ex, Pediatric Rash, Erythema Multiforme, Scalded Skin Syndrome, Molluscum, Eczema Herpeticum, Atopic Dermatitis), but let us look at one skin eruption that looks scary and is a great clue to other problems: Pyoderma Gangrenosum.
Many of us enjoy the aspect of medicine that requires our refined detective skills to not only find clues in the haystacks of chief complaints and presentations, but also use those clues to deduce a diagnosis. It is one of the unique characteristics of emergency medicine; however, when those clues are of dermatologic origin, they can be quite tricky. We have discussed several aspects of skin lesions previously (ex, Pediatric Rash, Erythema Multiforme, Scalded Skin Syndrome, Molluscum, Eczema Herpeticum, Atopic Dermatitis), but let us look at one skin eruption that looks scary and is a great clue to other problems: Pyoderma Gangrenosum.
Pyoderma Gangrenosum: What is it?
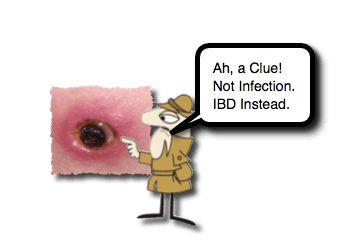
- This is a great example of a skin condition that can distract from the real problem.
- First described in 1916 (by a French Dermatologist, Louis Brocq) [Soleimani, 2016]
- Described as a rapidly progressive ulcer with a vertical ridge at the border, as sharp as a cliff.
- Had necrotic base with geometric edges.
- In 1930, Mayo Clinic group called it “pyoderma gangrenosum,” associating it with gangrene caused by strep infection.
- First described in 1916 (by a French Dermatologist, Louis Brocq) [Soleimani, 2016]
- Despite its appearance, it is not due to infection.
- It is on the spectrum of neutrophilic and autoinflammatory dermatoses. [Soleimani, 2016]
- Often initially misidentified as a pyogenic disease process.
- Characteristics:
- Pain is the major symptom. [Schoch, 2017]
- Appearance:
- May begin as pustules surrounded by erythema. [Schoch, 2017]
- Develop into the hallmark lesion: [Soleimani, 2016]
- Violaceous ulcer with overhanging/undermined, well-defined borders.
- Base is necrotic
- Contains granulation tissue and blood.
- May have purulent exudate.
- May involve subcutaneous and muscle layers.
- May begin as pustules surrounded by erythema. [Schoch, 2017]
- Can develop at sites of trauma
- Incidental bumps (also know as Pathergy) [Kechichian, 2017; Schoch, 2017]
- Surgical sites
- If not appreciated as pyoderma gangrenosum, surgeons may be consulted to debride….
- Debridement can worsen the lesion! [Soleimani, 2016]
- Can occur spontaneously also.
- Enlarge concentrically. [Kechichian, 2017]
- Location:
- Often on the lower extremities
- Most common presentation is disseminated ulcerative lesions on legs. [Kechichian, 2017]
- Kids have a higher involvement of the head and neck than adults. [Schoch, 2017]
- Often on the lower extremities
- It is uncommon.
- Which makes our vigilance necessary!
- Approximately 4% of cases occur in children. [Schoch, 2017; Kechichian, 2017]
Pydorema Gangrenosum: Think of…
- While it may look like it is overtly infected, it is actually a sterile lesion.
- More than 50% of lesions are associated with an underlying systemic illness: [Kechichian, 2017; Kechichian, 2017; Soleimani, 2016]
- Gastrointestinal
- Inflammatory bowel disease is the most frequent association in children
- Rheumatologic / Autoimmune
- ex, juvenile rheumatoid arthritis, arteritis
- Infectious
- ex, HIV, chronic hepatitis
- Hematologic / Malignancy
- ex, leukemias, monoclonal gammopathy
- Odd ball:
- Pyogenic Arthritis, Pyoderma gangrenosum and Acne (PAPA) Syndrome [Kechichian, 2017]
- Idiopathic – actually accounts for ~50% of cases [Kechichian, 2017]
- Gastrointestinal
Pyderma Gangrenosum: Diagnosis
- Diagnosis is often delayed. [Kechichian, 2017]
- It is a diagnosis of exclusion. [Kechichian, 2017]
- There is no specific serologic or radiographic markers for it. [Soleimani, 2016]
- Biopsy often performed to rule out other causes (ex, malignancy, infection, vasculitis).
- Neutrophilic dermal infiltration demonstrated.
- Other conditions to consider (abridged): [Soleimani, 2016]
- Infection
- Cutaneous anthrax
- Atypical myobacterium
- Traumatic ulceration
- Cutaneous malignancy
- Vascular insufficiency
- Behcet’s disease
- Vasculitis
Pyoderma Gangrenosum: Treatment
- There is no current gold standard of care. [Kechichian, 2017]
- Treatment is generally aimed at the underlying condition. [Kechichian, 2017]
- Main therapy is systemic steroids or other immunosuppressants/modulators. [Schoch, 2017; Soleimani, 2016]
- Most children have a good response to systemic steroids.
- Anti-tumor necrosis factor alpha agents are being used.
- Sulfasalazine is commonly used.
- Topical tacrolimus has also been used.
- If you are sending patient to a dermatologist, may want to withhold these medications as they may affect the ability to make the diagnosis.
- Surgical interventions are generally avoided, but…
- Can be helpful after the disease has been better controlled. [Soleimani, 2016]
- Biopsy, debridement, and grafting have been utilized.
Moral of the Morsel
- Not all “ugly” wounds are infected. It is important to consider infection, but if the kid has been on “100 courses” of antibiotics and not getting better… please think of another cause and Pydoderma Gangrenosum!
- A post-surgical ulcer that hasn’t responded to antibiotics may be pyoderma gangrenosum.
- Pyoderma Gangrenosum is just the “tip of the iceberg” (or ulcer of the inflammatory disease). Think about the potential associated conditions (particularly inflammatory bowel disease in children).
References
Schoch JJ1, Tolkachjov SN1, Cappel JA1, Gibson LE1,2, Davis DM1. Pediatric Pyoderma Gangrenosum: A Retrospective Review of Clinical Features, Etiologic Associations, and Treatment. Pediatr Dermatol. 2017 Jan;34(1):39-45. PMID: 27699861. [PubMed] [Read by QxMD]
Kechichian E1,2, Haber R1,2, Mourad N1,2, El Khoury R1,2, Jabbour S2,3, Tomb R2,4. Pediatric pyoderma gangrenosum: a systematic review and update. Int J Dermatol. 2017 May;56(5):486-495. PMID: 28233293. [PubMed] [Read by QxMD]
Soleimani T1, Sasor SE2, Spera L3, Eppley BE2, Socas J2, Chu MW2, Tholpady SS4. Pediatric pyoderma gangrenosum: is it just big wounds on little adults? J Surg Res. 2016 Nov;206(1):113-117. PMID: 27916349. [PubMed] [Read by QxMD]

[…] Strep, Scabies, Erythema Multiforme). Sometimes, though, things can get a little weird (ex, pyoderma gangrenous). Additionally, the child’s own skin conditions can influence the appearance of typical […]
[…] me being less than comfortable with all of the oddities that can present with skin findings (ex, pyoderma gangrenosum). This is why I approach rashes the way I do (see, Rash). Certainly, there are conditions that […]