![]()
Morphine and Appendicitis

Morphine and Appendicitis
“Don’t give the kid with potential appendicitis morphine!” the pediatric surgeon exclaims. Doing so will obscure their exam and delay the diagnosis… and that will make the surgeon angry… and you wouldn’t like it when the surgeon is angry.
We’ve all been taught this (or at least I was through several vivid experiences) and, while we know that it is not a valid case, the myth continues to persist.
The Myth
- Since the diagnosis of appendicitis is a clinical one, giving a medicine that can obscure the physical exam findings of appendicitis can confound the diagnosis and delay appropriate treatment.
- Actually I wholeheartedly agree that this diagnosis is clinical… why then are we asked about lab values constantly?
- Actually, this is another myth that should be addressed:
- No lab test is truly useful in ruling out the diagnosis… even the White Blood Cell Count
- As Amal Mattu taught me, “the WBC count is the last bastion of the intellectually destitute!”

- Delayed diagnosis leads to delayed treatment… delayed treatment leads to ruptured appendicitis.
- lInterestingly, now delayed treatment is even an option for some patients.
- Still, no one wants to have the appendicits progress to the point of rupture.
- By the transitive property (If a=b and b=c, then a=c) of medicine, Giving Morphine Leads to and Exploding Appendix.
The Truth
- Appendicitis hurts… we should make our patients more comfortable.
- The family brought the patient to you because the child was in pain… it is a little bewildering to the family to watch their child remain in pain while doctors continue to push on the area that hurts.
- This discomfort often leads to an appropriate response – reluctance to be evaluated!
- Studies have shown that morphine administered to patients who have a concerning clinical exam for appendicitis:
- Improves in their pain (shocking),
- Does not delay the diagnosis of appendicitis!
- Keeping the child calm and comfortable can actually improve the reliability of the physical exam.
Not that simple…
- Our pediatric surgeons are highly trained professionals with magical hands… so they can’t be completely off base… what continues to perpetuate the myth?
- Being overzealous with morphine can, certainly, lead to a near obtunded child who has an unreliable exam.
- If you need to do a jaw thrust to maintain the kid’s airway, determining whether there is tenderness over McBurney’s point might be difficult.
The Solution…
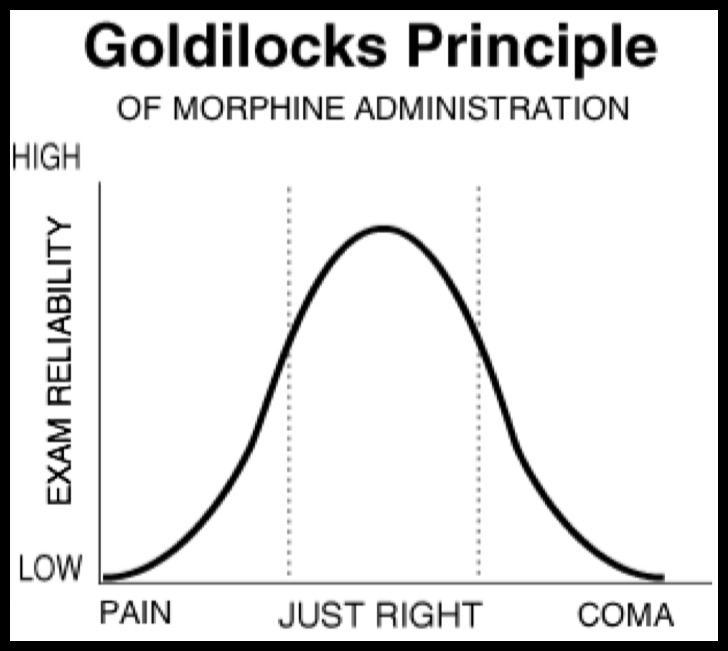
- The Golilocks Principle of Morphine administration – give the amount that is just right!
- Aim for the child to be more comfortable but not narcosed.
- This will make parents happy (and not having the parent march up and down my hallway makes me happy).
- This will also make your surgeon happy too… now the child does not just scream during the entire exam, but also is not unconscious.
- and… if the surgeon is not happy (perhaps even angry), then remind the surgeon that narcan can be given — but that he/she should explain that order to the family.
Yong Y, Jia-yong C, Hao G, Yi Z, Dao-ming L, Dong Z, Hui Z, Feng L. Relief of abdominal pain by morphine without altering physical signs in acute appendicitis. Chin Med J. 2010; 123(2): 142-145.
Anderson M. Analgesia for children with acute abdominal pain and diagnostic accuracy. BestBETs. 2008.
Author

[…] many medical “myths” previously (ex, Atropine for RSI, Cuffed ETTs, ORT vs IVF, Morphine for Appendicitis), but recently one of my esteemed PEM Fellows enlightened me about another. We have touched on […]
[…] direct our actions. By now, most of you know of my disdain for the ubiquitous WBC count (The Last Bastion of the Intellectually Destitute – Amal Mattu), but there is another often ordered test that may also fall into that category […]