![]()
Pseudosubluxation: Rebaked Morsel
Children love to trick us! Sometimes it is all in good fun and other times it is quite serious! They like to pretend to be well when they are truly sick (remember to check that Cap Refill and to never trust a Neonate!) and they often show us “odd” findings that are really normal (ex, Growth Plates, Primitive Reflexes). They like to keep us on our toes so much, that even their cervical bones can deceive us. Let’s recall one important morsel that deserves a Rebake – Pseudosubluxation of the pediatric cervical spine:
Pseudosubluxation: Basics
- Refers to the normal mobility of the cervical vertebrae, IN FLEXION, which may look to be pathologic but is not.
- Due to increased ligamentous laxity in this age group
- Occurs in children <8 yrs of age due to increased ligamentous laxity (> 8yrs, c-spine films should be similar to adults)
- Present at C2-C3 level (40%) or at the C3-C4 level (14%)
Pseudosubluxation: Determination of
- Must obtain good lateral cervical spine radiographs in flexion and extension
- The displacement should only occur in flexion (NOT extension)
- Most pediatric c-spine films are in flexion due to the occiput
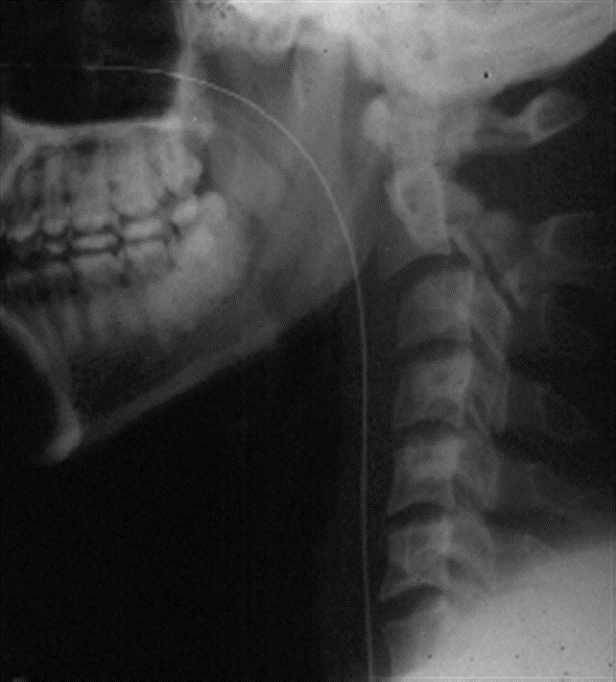
- Look at the Swischuk Line
- Line that is drawn from anterior aspect of C1-C3 spinous processes
- This line should be within 2 mm of the anterior aspect of the C2 spinous process
- Check the Spinal-Laminar Line
- The line drawn connecting the lamina of C1, C2, and C3 should remain intact even in flexion
- If you suspect that the misalignment represents pseudosubluxation, than you can reposition in extension and if the misalignment resolves, it is consistent with pseudosubluxation.
- Beware! The following may indicate a true subluxation-dislocation injury of fracture:
- If misalignment persists with extension of the neck
- If there is increased thickness of the pre-vertebral shadow which could indicate prevertebral swelling indicative of fracture (Note: this can occur sometimes with deep inspiration/ a screaming child or hypertrophied adenoids in children with no trauma history.)
- Loss of cervical lordosis
- Concerning mechanism
- Remember: CT will help identify bony injury, however MRI is the better test to assess for ligamentous injury as well as spinal cord injury
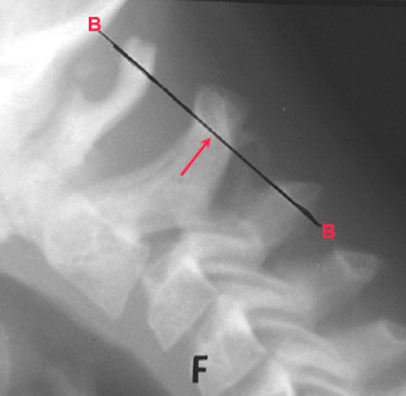
- Below is an example of a Hangman’s Fracture (See Cervical Spine Fractures).
Moral of the Morsel
- You eyes may deceive you! The cervical x-ray in children may appear to be abnormal, but that “subluxation” may not be true.
- Know your lines! Swischuk and the Spinal-Laminar lines will help you determine if this is a true problem or a pseudo-problem!
References:
Swischuk LE. Anterior displacement of C2 in children: physiologic or pathologic. Radiology. 1977 Mar;122(3):759-63. doi: 10.1148/122.3.759. PMID: 841068.
Kalanjiyam GP, Kanna RM, Rajasekaran S. Pediatric spinal injuries- current concepts. J Clin Orthop Trauma. 2023 Feb 4;38:102122. doi: 10.1016/j.jcot.2023.102122. PMID: 36846073; PMCID: PMC9945789.
www.Orthobullets.com
Author
